Accurate, thorough medical documentation is more than a best practice—it is a legal safeguard. In Mississippi, documentation issues are one of the most common reasons providers face scrutiny from the Mississippi State Board of Medical Licensure, the Mississippi Board of Nursing, and other regulatory bodies.
When records are incomplete, inconsistent, or misleading, they can raise concerns about patient care, billing practices, and overall compliance—often triggering a formal investigation or expanding the scope of an existing investigation.
The 9 Most Common Medical Documentation Mistakes
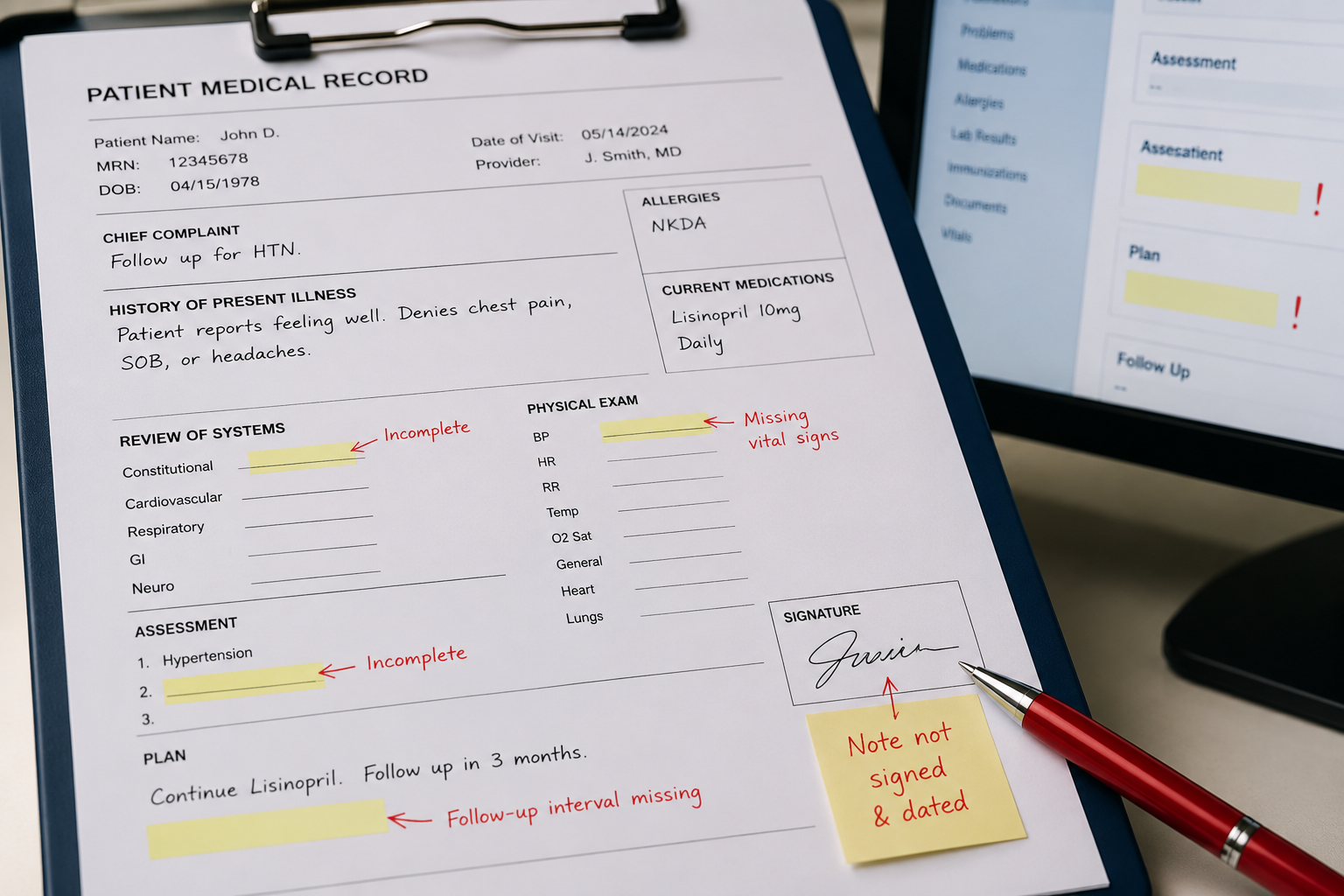
1. Incomplete or Missing Patient Records
One of the fastest ways to draw attention is by failing to document key aspects of patient care.
This includes:
- Missing histories or physical exam notes
- Lack of documented diagnoses
- Failure to record treatment plans or follow-ups
If it’s not documented, regulators often assume it didn’t happen.
2. Copy-Paste (Cloned) Notes
While electronic health records (EHRs) make documentation easier, overuse of copy-paste functions can create serious problems.
Risks include:
- Repeating outdated or incorrect information
- Identical notes across multiple patient visits
- Documentation that does not reflect actual care provided
Cloned notes are a major red flag during audits and investigations.
3. Inconsistent Documentation
Discrepancies within a patient’s record can quickly raise concerns.
Examples include:
- Notes that conflict with test results
- Differences between provider entries and nursing notes
- Mismatched timelines of care
Even small inconsistencies can suggest carelessness—or worse, intentional misrepresentation.
4. Poor or Illegible Entries
Although most records are now electronic, illegibility and unclear documentation still occur.
Issues may include:
- Vague or incomplete descriptions
- Unclear abbreviations
- Missing signatures or provider identification
Clear, professional documentation is essential for both patient care and legal protection.
5. Late Entries Without Proper Notation
Adding information after the fact is sometimes necessary—but it must be handled correctly.
Problems arise when:
- Entries are added or changed without noting the date/time of entry
- Documentation appears altered without explanation that an amendment or correction to an existing entry has occurred
Improper late entries can be viewed as an attempt to cover mistakes.
6. Lack of Medical Necessity Documentation
Clinical documentation must clearly indicate medical necessity for recommended treatment.
Investigations are often triggered or the scope expanded when:
- Services are not supported by appropriate documentation
- The medical necessity of a procedure or treatment is unclear
- Notes do not justify the level of care provided
This is a common issue in Medicare audits, which also indicate licensing concerns.
7. Failure to Document Informed Consent
Informed consent is critical—and it must be properly documented.
Missing documentation may involve:
- Lack of recorded risks and benefits discussion
- No patient acknowledgment or signature
- Failure to document alternatives to treatment
Without this, providers may be exposed to both legal and disciplinary action.
8. HIPAA and Privacy Documentation Failures
Documentation is not just about care—it also includes how patient information is handled under Health Insurance Portability and Accountability Act.
Common issues include:
- Accessing records without a valid reason
- Failing to protect against inappropriate disclosures of information
- Improper storage or transmission of records
Privacy violations can trigger both federal and state licensing penalties.
9. Lack of Follow-Up or Continuity of Care Notes
Patient care does not end after a visit—and your documentation shouldn’t either.
Red flags include:
- No follow-up instructions recorded
- Failure to document patient compliance or lack thereof
- Gaps in care coordination
These issues can raise concerns about patient safety and quality of care.
How Documentation Issues Turn Into Investigations
Documentation mistakes often come to light through:
- Patient complaints
- Insurance or government audits
- Peer review processes
- Internal reporting within hospitals or practices
- During a licensure investigation on another matter
What starts as a simple recordkeeping issue can quickly escalate into an expanded investigation—especially if patterns are identified.
How to Protect Yourself and Your Practice
To reduce your risk:
- Establish clear documentation protocols
- Regularly audit your own records
- Train staff on proper EHR use and disclosure
- Avoid over-reliance on templates and copy-paste
- Ensure billing aligns with documentation
Proactive compliance is one of the strongest defenses against investigations.
Protecting Your Medical and Nursing License in Mississippi
Documentation is often the foundation of any licensure investigation. Even minor errors can be misinterpreted when reviewed by regulators.
If your records are questioned or you are contacted by a licensing board, how you respond can significantly impact the outcome.
At Gilchrist Donnell, we help Mississippi health care providers navigate investigations, respond to documentation concerns, and protect their licenses and reputations. Give us a call for your confidential consultation.





